There is a connection of immune function with just about all nervous system disorders. The immune system is important not just for the nervous system, but for basically any disease in the body. Many diseases are due to chronic inflammation or the fact that the immune system attacks our own tissue. Any disease that results from such an aberrant immune response is termed an autoimmune disease.
The main component in nervous system disease is really “autoimmunity”. Such neuropathies as chronic inflammatory demyelinating polyneuropathy (CIDP), Guillain-Barré syndrome (GBS), and multifocal motor neuropathy (MMN) are caused by autoimmune mechanisms. Neurological autoimmunity can target virtually any structure within the central or peripheral nervous system and often in a highly specific way, targeting a very specific cell population.
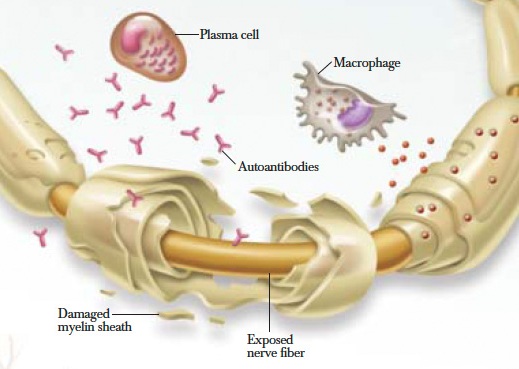
CIDP is the most common chronic inflammatory disease of the peripheral nerves, i.e. nerves outside the brain and spinal cord. An autoimmune attack on the myelin (insulation around individual nerve fibers, called axons) results in demyelination. Demyelination is the degeneration of fatty insulation covering the nerves (the myelin sheath). Loss of myelin can occur in sensory, motor or autonomic nerves. CIDP is a slowly progressive illness with diffuse sensory and motor symptoms.
The symptoms of CIDP begin with a combination of muscle weakness, as well as numbness and pain in the extremities. A person may also have impaired balance and difficulty walking as an early symptom. The disease usually begins in the legs but can begin in the arms at times. The disease can affect people of any age from childhood through one’s 80’s. Once the disease begins it typically progresses and can cause severe weakness and even death if left untreated.
In contrast, Guillain-Barre syndrome (GBS) patients develop rapidly progressive sensory symptoms such as unusual sensations (paresthesias) and numbness, and motor symptoms such as weakness and cramping in their legs followed by their arms. Patients may also develop weakness of their breathing and difficulty chewing and swallowing. GBS is considered the short-term variant. From the beginning of the disease and its initial weakness or fatigue to the eventual complete paralysis of the body, most likely takes place within a matter of hours or just a few days.
Multifocal motor neuropathy (MMN) is an inflammatory neuropathy related to an immune attack on motor nerves. It is a purely motor neuropathy affecting multiple motor nerves. MMN is a unique disorder characterized by slowly progressive, asymmetric, distal and upper limb predominant weakness without sensory loss.

Diagnosis, epidemiology and treatment of inflammatory neuropathies.
Chronic neuropathies – chronic inflammatory demyelinating neuropathy and its variants.
Research criteria for defining patients with CIDP.
Chronic inflammatory demyelinating polyneuropathy in common variable immunodeficiency.
Autoimmune neuromuscular disorders in childhood.
Multifocal motor neuropathy: diagnosis, pathogenesis and treatment strategies.
Today it is not known what causes autoimmune neuropathies, genetic factors are important, but is not the only explanation for development of an autoimmune neuropathy. Environmental factors, and also some infections, seem to be important as well. Infectious agents that can trigger autoimmunity include bacteria, yeast, and viruses like the Epstein Barr virus.
The autoimmune regulator plays a critical role in central tolerance by promoting thymic expression of self- antigens and deletion of self-reactive T cells. Thus, understanding these disorders ultimately requires an analysis of how the target antigen molecules affect immune cellular interactions both to generate the autoimmune reaction and to produce the immune–mediated injury of the nervous system.
It has been suggested that autoimmunity to peripheral myelin proteins is involved in the pathogenesis of CIDP and GBS. Mutations in myelin proteins (P0, P2 and PMP22) result in a wide spectrum of peripheral neuropathies, from congenital hypomyelinating to late onset sensory and motor axonal forms.
Altered protein level in the cerebrospinal fluid (CSF) is also a characteristic of patients with CIDP and GBS. A recent research shows that GBS is associated with low CSF index levels of prealbumin and fibrinogen, but normal levels of haptoglobin, whereas CIDP is associated with normal CSF index levels of prealbumin, low fibrinogen, and high levels of haptoglobin.
Immune responses to myelin proteins in Guillain-Barré syndrome.
Targeting of myelin protein zero in a spontaneous autoimmune polyneuropathy.
Viral and bacterial infections can cause indirect nerve damage by provoking conditions referred to as autoimmune disorders, in which specialized cells and antibodies of the immune system attack the body’s own tissues. These attacks typically cause destruction of the nerve’s myelin sheath or axon (the long fiber that extends out from the main nerve cell body).
For example, one theory about GBS involves complications following infection with Campylobacter jejuni, a bacterium commonly associated with food poisoning. This bacterium carries a protein that closely resembles components of myelin. The immune system launches an attack against the bacteria; but, according to the theory, the immune system confuses the myelin with the bacteria in some cases and attacks the myelin sheath as well.
Infection with certain viruses is also associated with neuropathies. Neuropathy can result from severe vasculitides, a group of disorders in which blood vessels are inflamed. When the blood vessels are inflamed or damaged, blood supply to the nerve can be affected, injuring the nerve.
The neurotropic herpes viruses: herpes simplex and varicella-zoster.
Varicella-zoster virus vasculopathy: immune characteristics of virus-infected arteries.
Neurologic manifestations of varicella zoster virus infections.
As with many neuropathy cases, neurotoxin overload is a common problem that affects many patients. Neurotoxins are substances attracted to our nervous system. They are absorbed through the nerve endings and travel inside the neuron to the cell body. Along the way, they disrupt many nerve cell functions vital to life. The source of neurotoxins may be heavy metals, viruses, bacteria, fungi, molds, parasites and protozoa.
Hihg vitamin intake can also produce neuropathy. Vitamin A toxicity is a good general model of vitamin neurotoxicity, because it shows the importance of the ratio of vitamin and vitamin-binding proteins in producing vitamin toxicity and of CNS permeability barriers. The neurological effects of vitamin deficiency and vitamin excess are similar. There are individual differences in susceptibility to vitamin neurotoxicity, and ordinary vitamin doses may harm occasional patients with genetic disorders.
Many bacteria are able to produce enterotoxins or toxins. The digestive tract is one of the ecosystems that harbors the largest number and greatest variety of bacteria. Among them, certain bacteria have developed various strategies, including the synthesis of virulence factors such as toxins, to interact with the intestinal mucosa, and are responsible for various pathologies.
Various enterotoxins interact with the enteric nervous system, for example by stimulating afferent neurons or inducing neurotransmitter release from enterochromaffin cells which result either in vomiting, in amplification of the diarrhea, or in intestinal inflammation process. Other toxins pass through the intestinal barrier and disseminate by the general circulation to remote organs or tissues, where they are active, and can pass the blood brain barrier and directly act on specific neurons.
Toxins act on the body’s cells, tissues, and organs and interfere with important body processes, thereby interrupting normal body functions. Toxins interfere specifically with key components of critical functions in eukaryotic cells, such as enzyme or hormone receptors on the cell surface or intracellular regulatory proteins. Also, in response to toxins, the body produces special antibodies called antitoxins, which unite with and neutralize the toxins, providing defense against disease.
Medication, toxic, and vitamin-related neuropathies.
Therefore, the health of the gut bacteria is critical for the immune system. There are literally trillions of bacteria in the gut, and one of their jobs is to regulate the immune system. Gut bacteria influence also development of the CNS and stress responses. Furthermore, the gut is quite literally the second brain, as it originates from the same type of tissue (neural crest) as the brain. During fetal development, one part turns into the CNS, while the other develops into the enteric nervous system (ENS).
These two systems are connected via the vagus nerve, the tenth cranial nerve that runs from the brain stem down to the abdomen. The vagus nerve has also emerged as an important means of communicating signals from gut microbes to the CNS. The brain-gut axis involves interactions among the neural components, including (1) the autonomic nervous system, (2) the central nervous system, (3) the stress system (hypothalamic-pituitary-adrenal axis), (4) the (gastrointestinal) corticotropin-releasing factor system, and (5) the intestinal response (including the intestinal barrier, the luminal microbiota, and the intestinal immune response).
Hence the gut flora, gut and brain work in tandem, each influence the other (the microbiota-gut-brain axis). And this is why the intestinal health can have such a profound influence on the nervous system. This also helps explain the link between neurological disorders (including ADHD and autism) and gastrointestinal dysfunction. The CNS is closely linked to the immune system at several levels.
Thus, an altered immune modulatory balance on nerve cells can be driven by both top-down (ie, CNS pathology) and bottom-up (ie, intestinal immune activation) influences. Dysregulation of the innate and adaptive immune system directed against luminal bacteria or their products found in the intestinal lumen and inappropriate immune responses to organisms in the intestine that normally do not elicit a response, possibly because of alterations in the microbiota-gut-brain axis function.

Biology of the adult enteric neural stem cell.
The interplay between the intestinal microbiota and the brain.
The microbiome-gut-brain axis: from bowel to behavior.
On communication between gut microbes and the brain.
The role of probiotics and antibiotics in regulating mucosal inflammation.
Brain-gut interactions in inflammatory bowel disease.
Experimental endotoxemia as a model to study neuroimmune mechanisms in human visceral pain.
Immune system in the brain: a modulatory role on dendritic spine morphophysiology?
Neuro-immune crosstalk in CNS diseases.
Immune activation in the small intestine in patients with rheumatoid arthritis.
In recent decades, our gut flora has been damaged by antibiotics, toxins and by the modern western diet. Imbalance in the gut flora has been shown to directly increase the risk for autoimmunity and other immune disorders. There is growing evidence that increased intestinal permeability plays a pathogenic role in various autoimmune diseases. The overall composition of the microbiota or exposure to specific bacterial strains can modulate neural function, peripherally and centrally. Healthy gut bacteria can provide protection from the central effects of infection and inflammation as well as modulate normal immune responses.
Yet conventional medicine doesn’t take these factors into account when treating autoimmune neuropathies. Instead, it tries to shut down the immune response with powerful medications including nonsteroidal anti-inflammatory drugs (NSAIDs), steroids, immunosuppressive drugs, and new drugs that block the effects of a powerful inflammatory molecule called TNF alpha.
These drugs shut down the immune system so powerfully that they increase the risk of cancer or life-threatening infections. And they have frequent and serious side effects and often give only partial relief. These drugs may be lifesaving for some in the short run — but in the long run they do nothing to deal with the causes.
Our approach to treating autoimmune neuropathy patients is to optimize their immune function which requires optimization of every other body system. We have successfully treated 2 CIDP patiens with Hepazym plus Ginolzym therapy. CIDP and MMN might be controlled and even cured without drugs by this therapy.


{kind=link}