Many scientists believe that microbes cause or contribute to between 15-25% of all cancers diagnosed worldwide each year. The frequency of liver cancer is high among Asians because liver cancer is closely linked to chronic hepatitis B infection. This is especially so in individuals who have been infected with chronic hepatitis B for most of their lives (it is usually a childhood disease). HBV infection is a serious clinical problem because of its worldwide distribution and potential adverse sequelae. Nearly 300 million persons in the world are chronically infected with hepatitis B virus. High rates of chronic infection are found in some parts of Asia, Africa, the Pacific islands, South America, and the Middle East.
Although HBV can survive outside the body for up to 1 week—and therefore, might be transmitted via indirect contact, such as from open sores—hepatitis B is spread predominantly parenterally, through intimate personal contact, and perinatally. Individuals at risk include intravenous drug users, children of mothers with HBV, men who have sex with men, patients on hemodialysis, and those exposed to blood or blood products.
Because infection usually persists for many years, if not lifelong, HBVs need efficient mechanisms to hide from the immune response of the host. HBVs are prototype non-cytopathic viruses causing persistent infection. Cytopathic effect (CPE) is structural changes in a host cell resulting from viral infection. CPE occurs when the infecting virus causes lysis (dissolution) of the host cell or when the cell dies without lysis because of its inability to reproduce.
As HBV is not cytopathic by itself, chronic HBV infection is a dynamic state of interactions between the virus, hepatocytes and the host immune system. Accordingly, the natural course of chronic HBV infection can be divided into three phases: (i) immune tolerance, (ii) immune clearance and (iii) residual or inactive phase. Immune tolerance phase is characterized by high HBV replication with little clinicopathological changes. During the immune clearance phase, hepatitis activity and even hepatitis flares with serum ALT (alanine aminotransferase) over five times upper limit of normal (ULN) may occur, and these may sometimes be complicated by hepatic decompensation.
To escape the immune response, they exploit different strategies. Firstly, they use their structural and non-structural proteins multiplely. One of the purposes is to alter the immune response. Secondly, they replicate by establishing a pool of stable extrachromosomal transcription templates, which allow the virus to react sensitively to changes in its microenvironment by up- or downregulating gene expression. Thirdly, HBVs replicate in the liver which is an immunopriviledged site.

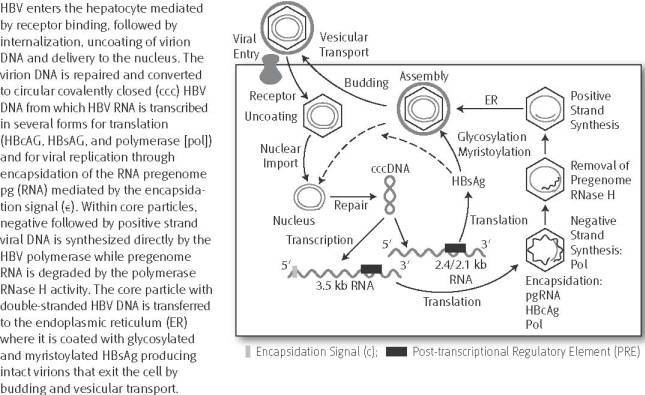
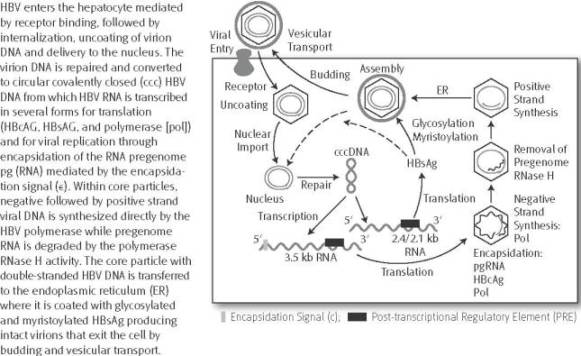
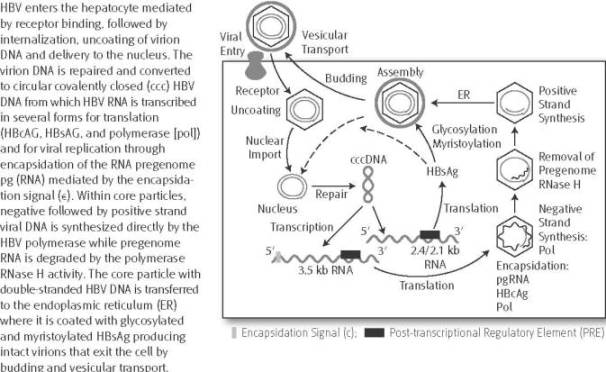
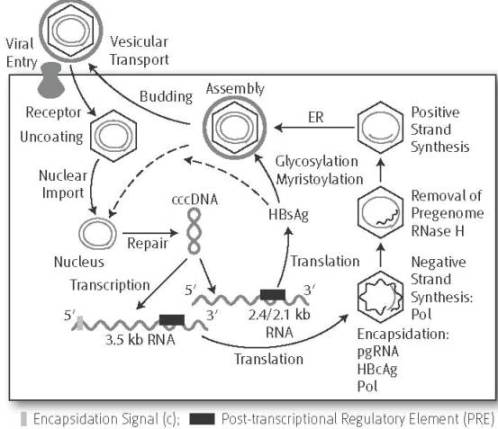
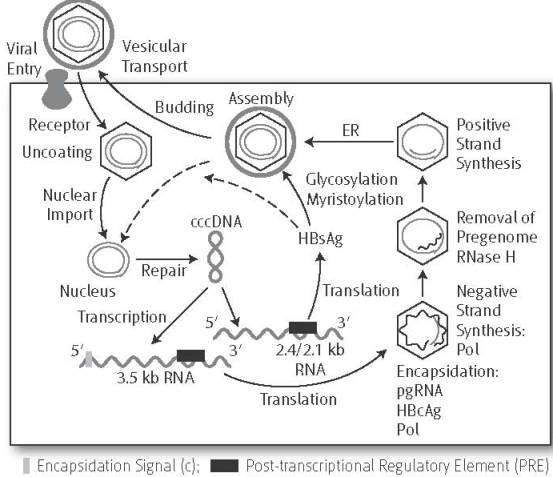
HBV life cycle: HBV enters the hepatocyte mediated by receptor binding, followed by internalization, uncoating of virion DNA and delivery to the nucleus. The virion DNA is repaired and converted to circular covalently closed (CCC) HBV DNA form which HBV RNA transcribed inseveral forms for translation (HBcAg, HBsAg and polymerase [pol]) and for viral replication through encapsidation of the RNA pregenome pg (RNA) mediated by encapsidation signal. Within core particles, negative followed by positive strand viral DNA is synthysized directly by the HBV polymerase while pregenom RNA is degraded by the polymerase RNase H activity. The core particle with double-stranded HBV DNA is transferred to the endoplasmic recticulum (ER) where it is coated with glycosylated and myristoylated HBsAg producing intact virions that exit the cell by budding and vesicular transfort.
Chronic hepatitis B virus infection in Asian countries.
Transmission of occult hepatitis B virus by transfusion to adult and pediatric recipients in Taiwan.
Chronic infections with hepatotropic viruses: mechanisms of impairment of cellular immune responses.
Immune escape by hepatitis B viruses.
Chronic hepatitis B is defined as the presence of HBsAg in the serum of a patient that persists for at least 6 months. HBsAg is the “surface antigen” of the Hepatitis B Virus (HBV). It indicates current Hepatitis B infection. Patients who developed antibodies against HBsAg (anti-HBsAg seroconversion) are usually considered non-infectious. The immune system maintains an “immunological memory” against past pathogens to facilitate early detection and to confer protective immunity against a rechallenge. This explains why many childhood diseases never recur in adulthood. Seroconversion is the development of antibodies detectable in the serum, after exposure to a particular organism or antigen, in a person who was previously immunologically ‘naive’ for–ie, previously unexposed to a particular antigen. These are generally the last antibodies to appear. HBsAb can neutralise the hepatitis B virus and there appearance taken as an indicator that an initial infection has been defeated.
Chronic hepatitis B seroconversion is rare. The clearance of circulating hepatitis B surface antigen (HBsAg) and appearance of antibody (HBsAb) to HBsAg have been generally accepted as evidence of clinical and serologic recovery from chronic hepatitis B virus infection. HBsAg clearance in chronic Hepatitis B is delayed and infrequent: 1-2% per year in Western countries where HBV infection is usually acquired in adulthood; 0.05%-0.8% per year in endemic areas where HBV infection is mostly acquired vertically.
HBeAg stands for hepatitis B “e” antigen. This antigen is a protein from the hepatitis B virus that circulates in infected blood when the virus is actively replicating. The presence of HBeAg suggests that the person is infectious and is able to spread the virus to other people. HBeAb stands for ‘e” antigen antibody. Antibodies to the ‘e’ antigen (HBeAb) normally appear a few weeks after HBeAg is no longer detectable. The presence of HBeAb is generally taken to be a good sign and indicates a favourable prognosis.

It is clear that sustained viral suppression is the key to the reduction or prevention of hepatic injury and disease progression. Therefore, the primary goal of treatment for chronic hepatitis B is to eliminate or permanently suppress HBV. This will decrease pathogenicity and infectivity, and thereby stop or reduce hepatic necroinflammation. In clinical terms, the short-term goal of treatment is to ensure HBV-DNA sustained suppression, ALT normalization and prevent the development of decompensation (initial response), to reduce hepatic necroinflammation and fibrosis during and after therapy (maintained and sustained response). The ultimate long-term goal of therapy is to eliminate HBV viruses to prevent progression to cirrhosis and/or liver cancer, and to prolong survival (durable response).
The infected hepatocytes are identified and eliminated by cytotoxic T lymphocytes and the balance between Th1 cells and Th2 cells play an important role in the hepatocyte damage. Two stimulating signals are necessary for the activation of T lymphocytes. One comes from the specific binding of T cell receptor (TCR) to the complex of major histocompatibility complex (MHC) molecules and antigen peptide and the other is provided by bind antigen presenting cells to the adhesion molecules on the surface of T cell.

Unfortunately, there is no cure for hepatitis B. Not only chronic hepatitis B but also chronic hepatitis C may eventually cause liver cirrhosis and liver cancer, a fatal disease with very poor response to current chemotherapy. The best treatment includes rest and proper diet.
Diagnosis of hepatitis B virus infection through serological and virological markers.
Implication of Th17 and Th1 cells in patients with chronic active hepatitis B.
Modulation of the immune response mediated by dietary nucleotides.
Hepazym is one of the most powerful natural immune modulator/enhancer developed for treatment of patients with chronic hepatitis B (HBV) and chronic hepatitis C (HCV). Hepazym activates following pathways.
Association of interleukin-18 gene polymorphisms with hepatitis B virus clearance.
Hepazym contains an “adaptogenic” mixture of fermented herbal compounds including fermented medicinal mushrooms, plant enzymes, plant sterols, lactose, antioxidants and polyphenols in a synergistic proprietary formula designed to promote anti-HBV and anti-HCV effects. Medicinal mushrooms grown on natural sources enzymatically activate a process whereby complex cross-linked polysaccharides from the vegetable sources are converted to biologically active immunomodulators (also known as biological response modifiers).
The polysaccharides produced by enzymatic fermentation process are effective and safe immune stimulants. Hepazym can modulate positively or negatively the biological response of immune cells. Hepazym contains certain mushroom derived-glucans and polysaccharide-bound proteins which have been shown to act as immunomodulators, where these polymers interact with the immune system to upregulate or downregulate specific aspects of the responses of the host and this may result in various therapeutic effects. Whether certain compounds enhance or suppress immune responses can depend on a number of factors including dosage, route of administration, timing and frequency of administration, mechanism of action or the site of activity.
In recent two clinical trials, Hepazym daily dosing 60 ml (20 ml 3 times per day) has been used to treat chronic HBV patients. Hepazym has been shown to be active in patients with: HBeAg+, HBeAg-, and lamivudine resistant HBV. Hepazym has shown durable HBV DNA suppression with a high threshold for the development of resistance. 2 patients achieved HBsAg seroconversion with Hepazym monotherapy after a median of 16 weeks. HBsAg seroconversion was durable off treatment. All patients with HBsAg seroconversion maintained undetectable HBV DNA and normal ALT levels off treatment.
When it comes to diet, it is very important to avoid eating toxins and pesticides. Hepatitis patients rarely have organic foods. Contrary to what most people believe, “organic” does not automatically mean “pesticide-free” or “chemical-free”. So what does organic mean? Organic foods are produced without the use of chemicals, herbicides, fungicides, petroleum-, sewage- or sludge-based fertilizers or chemical pesticides. Organic food is not bio-engineered, genetically modified, nor is it irradiated. Poultry and Beef are fed only organic feed, are grazed on organically maintained pastures, and are not given antibiotics, hormones or animal by-products.
Sweet potato (Ipomoea batatas) is an important crop and a major source of starch worldwide; therefore, there is a wide interest in studying the mechanisms it uses to protect against environmental stresses. The expression of the IPO (ipomoelin) gene in sweet potato was shown to be enhanced by the application of methyl jasmonate (MeJA) and mechanical wounding. Together, H2O2 and NO regulate the expression of the IPO gene, and their interaction might further stimulate plants to protect themselves from invasions by pathogens and herbivores.
Sweet potato leaves provide a dietary source of vitamins, minerals, antioxidants, dietary fiber, and essential fatty acids. Bioactive compounds contained in this vegetable play a role in health promotion by improving immune function, reducing oxidative stress and free radical damage, reducing cardiovascular disease risk, and suppressing cancer cell growth. Study showd that consumption of sweet potato leaves modulates various immune functions including increased proliferation responsiveness of PBMC (peripheral blood mononuclear cells), secretion of cytokines IL-2 and IL-4, and the lytic activity of NK cells.
Consumption of purple sweet potato leaves decreases lipid peroxidation and DNA damage in humans.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}