Sulfur, after calcium and phosphorus, is the most abundant mineral element found in our body. It is available to us in our diets, derived almost exclusively from proteins, and yet only 2 of the 20 amino acids normally present in proteins contains sulfur. The sulfur-containing amino acids (methionine and cysteine) are found principally in red meat and dairy products. Proteins contain between 3 and 6% of sulfur amino acids. A very small percentage of sulfur comes in the form of inorganic sulfates and other forms of organic sulfur present in foods such as garlic, onion, broccoli, etc.
The metabolism of both sulfur containing amino acids is closely related. Methionine is one of the essential amino acids with many key roles in mammalian metabolism. It is a precursor for cysteine formation in human liver. Cysteine is classified as semiessential due the variable capacity of the body for its production from methionine. Methionine, although it cannot be regenerated from cysteine, can be recycled through methylation of homocysteine using a single carbon (methyl-) donor such as betaine (from choline), folate, or vitamin B12 (Cobalamin).
Sulfur is both crucial to life and a potential threat to health. One significant change in the modern diet in areas with high incidence of inflammatory bowel disease (IBD) is the high intake of sulfur-containing food. Sulfur not recycled by an intestinal sulfur salvage pump passes into the colon where it is metabolized, in some, by sulfate-reducing bacteria (SRB), a group of bacteria identified as being much more common in individuals with UC and associated with flares of UC, in particular.
Many bacteria reduce small amounts of sulfates in order to synthesize sulfur-containing cell components. By contrast, the sulfate-reducing bacteria (SRB) reduce sulfate in large amounts to obtain energy and expel the resulting sulfide as waste. Hydrogen sulphide is a by-product of H(2) metabolism by SRB, which are ubiquitous in the colonic mucosa.
Hydrogen sulfide (H2S) is a gas that is toxic in large quantities, but safe in lower quantities for those who are not in vulnerable groups and have developed tolerances. Although higher hydrogen sulphide (H2S) and SRB levels have been detected in patients with IBD, and to a lesser extent in colorectal cancer, this colonic gas might have beneficial effects.
Are we getting enough sulfur in our diet?
Microbial pathways in colonic sulfur metabolism and links with health and disease.
Emerging role of hydrogen sulfide in colonic physiology and pathophysiology.
Hydrogen sulfide in gastrointestinal and liver physiopathology.
Impaired detoxication of hydrogen sulfide in ulcerative colitis?
Hydrogen sulfide is an endogenous potentiator of T cell activation.
Some of the large intestine bacteria convert the soluble fiber and resistant starch that are present in undigested food into short-chain fatty acids (SCFAs). One of these fatty acids, called butyric acid, has important health benefits in the colon (the longest section of the large intestine). Green bananas contain a large quantity of resistant starch, which some bacteria can change into butyric acid.
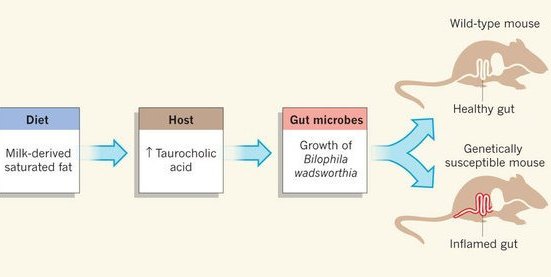
Some foods contain relatively high concentrations of butyric acid, including butter and parmesan cheese. Butter contains 3% to 4% butyric acid. Kombucha tea also contains butyric acid. However, butter also contains longer chained, less healthy fatty acids and consumption of a diet high in saturated (milk-derived) fat, but not polyunsaturated (safflower oil) fat, can trigger IBD by encouraging the growth of one bacterium in particular, Bilophila wadsworthia, to about six percent of the total bacteria.
Functional interactions between the gut microbiota and host metabolism.
Dietary-fat-induced taurocholic acid promotes pathobiont expansion and colitis in Il10-/- mice.
Butyric acid helps maintain a healthy intestinal lining and has also relieved symptoms in people with inflammatory bowel disease (IBD). In addition, butyric acid lowers the risk of colon cancer. Butyric acid provides the primary fuel for colonocytes. Proper ion transfer, mucus synthesis, phase II detoxification, and lipid synthesis for cell membrane integrity in the colonocytes depend on butyrate oxidation. Impaired metabolism of SCFAs has been implicated as a factor in IBD.
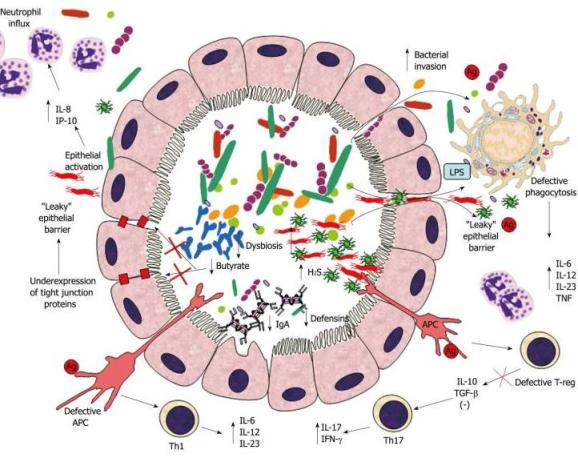
Hydrogen sulphide (H2S) has been shown to inhibit the butyrate oxidation in colonocytes. Study shows that patients with active IBD have significantly lower butyrate oxidation than patients in remission. Because normal oxidation was observed in patients in remission, faulty SCFA oxidation is likely to be a result rather than a primary cause of IBD. High concentrations of SRB with concomitant elevation of hydrogen sulfide (H2S) have been noted in patients with IBD. Therefore, hydrogen sulfide (H2S) can potentially damage the gut mucosa by inhibiting butyrate oxidation in the mitochondria, essentially starving the colonocyte.
Intestinal microbiota in inflammatory bowel disease: friend of foe?
Butyrate and the colonocyte. Implications for neoplasia.
Butyrate and glucose metabolism by colonocytes in experimental colitis in mice.
Effect of butyrate enemas on the colonic mucosa in distal ulcerative colitis.
Methionine is usually found in greater amounts in eggs, fish, red meat, processed meat and dairy products. High dietary intakes methionine (5–6 g/day) on the other hand has been shown to raise plasma levels of homocysteine, despite adequate intakes of B vitamins. Homocysteine is a sulfur-containing, nonproteinogenic amino acid that is an intermediate in methionine metabolism. This raises some concern as one does not want to activate the immune system at the cost of enhancing monocyte adherence to endothelial cells. High homocysteine increases pain and inflammation.
Furthermore, in a study, markedly elevated concentrations of homocysteine in the colonic mucosa were observed in patients suffering from UC and CD. Increased homocysteine levels in the colonic mucosa and plasma of patients with IBD may play a role in the pathogenesis of UC and CD.
The effects of sulfur amino acid intake on immune function in humans.
Summary: Nutritional factors are important in IBD. The factors currently believed to help prevent or treat IBD are as follows:
GinolZym contains butyrate, a short chain fatty acid (SCFA) that is a potent detoxifier of ammonia and neurotoxins. Butyrate is the single biggest metabolite of fiber. It encourages the formation of friendly bacteria in the gut. Furthermore, GinolZym has an inhibitory effect on most of harmful bacteria in the gut.




{kind=link}
{kind=link}